Ida Bafende talks to DrB about habit reversal for childhood atopic eczema

IB: Although for a few their eczema seems relatively mild, for the majority it is quite severe, and longstanding. The main struggles for many of them are with the seemingly constant scratching, and with skin infections. These difficulties are irrespective of age. Many of the children seem never completely clear of their eczema. An important aspect of my work is to ensure that my patients understand all they need about their eczema, and how to get the most benefit from the recommended treatment.
DrB: How did you come to hear about The Combined Approach and habit reversal? Why did you decide to use this programme for one of your patients?
IB: The habit reversal treatment programme was mentioned to me by one of my consultants. Then I was really happy to attend the multidisciplinary meeting devoted to the topic last year. It was really fascinating. The outcomes reported were amazing. I realised the programme could work really well for some of my patients, especially those who were struggling with constant scratching.
DrB: Did you find the programme easy to understand? How much preparation was required before you saw your first patient?
IB: The programme is very easy to understand. The steps are clearly explained, both in Atopic Skin Disease - Manual for Practitioners and in the articles on this website. As a health care professional, after coming to the meeting I knew generally what would be involved, but it was important to familiarise myself with the details, so that I could then maximise a natural flow of discussion during clinic visits. For me, this was very important. I wanted my patient and her mother to feel comfortable and at ease - and not to seem as if I was speaking from a script, like a robot!
DrB: Tell us then a little about the first patient you saw for The Combined Approach. Why did this patient seem appropriate for this programme? How was the patient’s eczema when you started? How easy was it to give the patient the first homework task to follow?
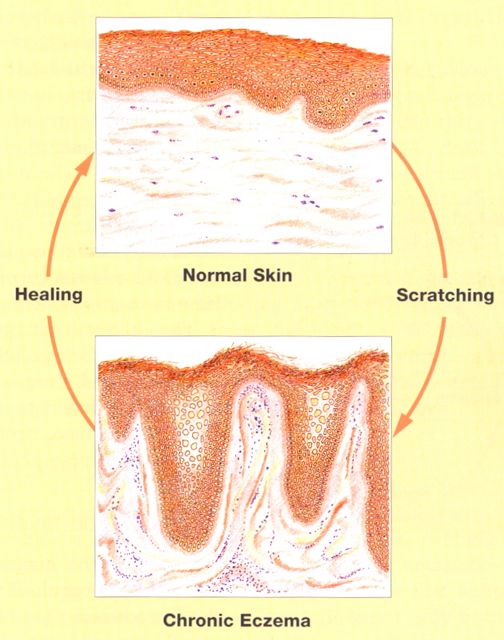
IB: My first patient had over several years been a regular attender at one of my Consultant’s outpatient clinics. Her eczema seemed hard to treat. She was now 12 years old, and very willing and keen to discuss a new treatment approach, and her mother was willing and committed to help and support her. She seemed a perfect match for the version of the habit reversal programme for older children. At her first visit, her face was very dry but only mildly eczematous. Her neck, flexures, wrists, and hands were moderately affected by chronic eczema, with evidence of regular scratching - with both scratch marks, or excoriations, and skin thickening, or lichenification. Her mother remarked she often seemed to scratch absent-mindedly, without knowing what she was doing. She herself spoke of embarrassment and lack of confidence, linked to how she thought her skin looked to others. Even in hot weather she would wear long sleeves to cover up her eczema, especially at school. She spoke of wanting to feel confident enough to wear short sleeves again. It was very easy to give her instructions for her first homework, Registration, or “awareness training”: how to use a hand-tally counter to make her aware of her scratching, by counting her scratching frequency, and keeping a record of her daily totals, together with a list of situations when scratching was most often happening. She agreed that her mother could help her: when her mother saw she was scratching, I suggested now her mother could say to her “Click!”, rather than “Don’t!”. During the week between the first two appointments she continued as before with her usual treatment. The patient handbook we gave her covers all that was involved, and it is easy to understand. She quickly knew what she needed to do, and was very willing to do it.
DrB: At the second visit, what did the patient say she had discovered? What was your main task during this appointment?
IB: After a week using a hand tally counter to count her scratching she said she now realised that she was scratching much more than she had previously thought, and certainly not all was due to itch. On one day she had recorded a total of 160 scratching episodes. This was a real surprise to her. She estimated 80% of her scratching at least started because of itch. She could see at least 20% of all her scratching started without any itch at all. The early mornings, the early evenings and when she was not busy doing things, all seemed to be times when most scratching happened. My main tasks now were to reassure and encourage her, and to help her to understand how her scratching behaviour could be changed, and to understand how to clear her skin of chronic eczema by her own efforts.
DrB: At this second visit then you introduced her to the three levels of treatment of The Combined Approach?
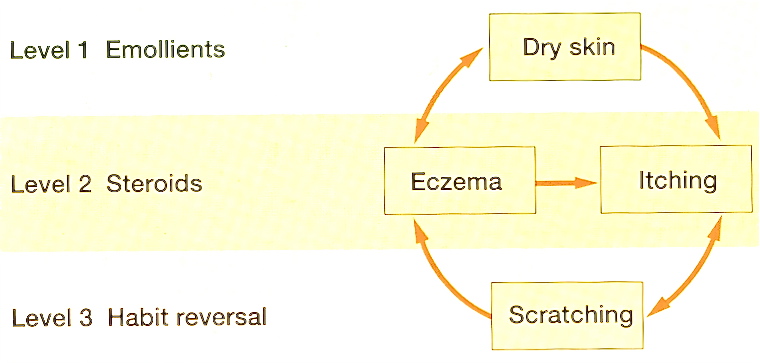
IB: Yes, that’s right. First of all her regime of emollients and topical steroids was reviewed, to ensure it was understood and was optimal. Then, the programme principles for scratching prevention, or habit reversal were given, together with a demonstration of what to do, for her to copy. She was also especially encouraged to devise strategies that would be particularly helpful to her. She was now aware of her scratching “danger times”. She was encouraged to have a plan that would enable her to put in place alternative activities that would keep her skin safe and allow natural healing: what are called “skin-safe behaviours”. She could usefully discuss her plan with others, and write it in her handbook.
DrB: Tell us about your patients progress. What did you need to do to help, and what did she do to help herself?
IB: At her third appointment after two weeks' treatment she was already delighted: her progress was clear. Not only had the frequency of scratching episodes reduced, her mother said what she was doing when she scratched had changed - she had become much less aggressive. After only one week of the programme she was sleeping through the night without anti-histamines. She had used the habit reversal as taught, and a friend at school had suggested she could use a fidget-toy as a skin-safe behaviour. She was encouraged to continue as she was going, with now a focus on habit reversal each day, to get maximum natural healing, alongside the benefits of her continuing topical treatment.
DrB: Usually in clinic there are four visits over about 5 weeks to complete The Combined Approach to arranging follow-up. How was it for your patient? What was the outcome? What was the follow-up plan?
IB: Because of school holidays she came back for her fourth appointment after another 3 weeks. With continuing use of her creams, and with focused habit reversal, her eczema had quickly cleared. Both she and her mother said that her skin had not been so clear for such a long time. Now she was counting only about 20 scratching episodes a day, and now mostly just touching her skin, rather than any real scratching. And there was much less itch. Her quality of life had really improved: she was now especially happy to be wearing short sleeves again, and to able to swim in the sea without her skin stinging! For follow-up treatment now we agreed she no longer needed habit reversal, nor regular anti-inflammatory cream treatments: she was advised how to continue to use her emollients, and given advice about recognising acute flare-ups and their effective treatment. We agreed her usual follow-up outpatient appointment with her Consultant Dermatologist could be cancelled, and a longer term appointment with me was made to ensure all was going according to plan.
DrB: Do you think The Combined Approach can be a success for other children with eczema that come to your clinic? If so, in what way? What can you see as possible difficulties, if any, in offering this programme? What tips can you share on how to go about using the programme successfully in an outpatient clinic like yours.
IB: Yes, I do think there are other children who will benefit from The Combined Approach. Absolutely. However, the success of the programme will depend on adjusting the programme to the age of the child, plus their ability, willingness and commitment to being helped in this way, and also their parents’ commitment and involvement too! To use the programme in our clinic successfully, there has to be an agreed capacity to see children at the appropriate time intervals. And the time spent with both child and parent cannot be rushed - plenty of time needs to be put aside. But the long-term benefits will be very much worth the time spent in the short term.
DrB: Thank you. Can we get back in touch with you to follow the progress of your patient?
IB: Yes, of course: I look forward to that - and I will keep in touch with you all at atopicskindisease.com. Thank you.
References
Noren, P & Bridgett, C (2017) Habit reversal and chronic atopic eczema in childhood. Patient Information Leaflet. Nottingham Support Group for Carers of Children with Eczema
If you have questions for Ida Bafende, please ask them below...
SEE ALSO